MASS Design Offers Guidance for Adapting Hospitals on the Fly
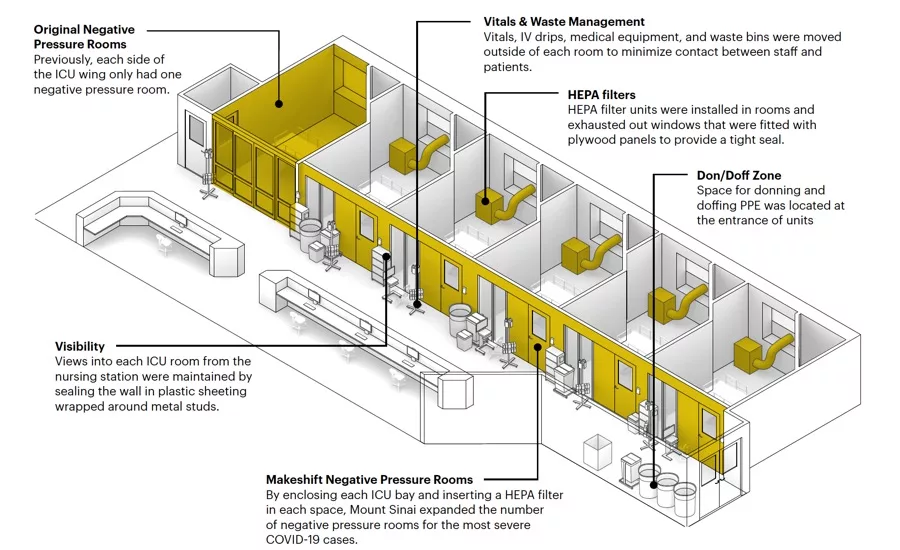
Diagram of interventions on the Guggenheim Pavilion
Image courtesy MASS Design Group and Ariadne Labs
Architects & Firms
Public health officials in cities around the world have used the phrase “flattening the curve” endlessly during the pandemic to encourage behavior that would help prevent a massive wave of COVID-19 patients from converging on hospitals all at once. When that wave threatened to break, becoming a frightening reality in New York and other cities, hospitals scrambled to add acute care beds as fast as possible.
Boston’s MASS Design Group, with Ariadne Labs—a health-systems innovation center founded by Atul Gawande, the surgeon and New Yorker writer—collaborated with Mount Sinai Hospital in Manhattan to help manage the surge. Their task was to protect health workers on the front lines as rooms and suites were drastically transformed.
With so little definitively known about the behavior of the coronavirus, “We’re wrestling with ambiguities about how to manage infection control, separate infectious patients, and assure health-worker safety,” said MASS co-founder Michael Murphy. The partners worked with infection prevention, clinical operations, and facilities teams at Mount Sinai via video conferencing to adapt existing spaces for COVID-19 patients. Head-mounted GoPro cameras allowed the designers to track staff workflow in spaces they were not allowed to visit. Bringing together what the larger team learned, MASS has now released “Redesigning Hospital Spaces on the Fly to Protect Health Workers” (PDF), an online case study of Mount Sinai’s response, available for free to all. The firm brought unique insights from its work in developing countries that have struggled with infectious diseases, including Haiti and Rwanda.
Since Mount Sinai retrofitted entire suites, not just individual rooms, the guidance focuses to a considerable extent on helping caregivers find their way through bafflingly labyrinthine environments temporarily configured to isolate those exposed or infected. Paint, signage, and tape (green or red) applied to the floor alert staff to the level of risk they encounter as they pass through a corridor or into a patient room. Such wayfinding measures also remind people of when they must clean hands and where they must wear personal protective equipment, or PPE, such as gowns, caps, and masks. The team learned that the greatest risk-heightening confusion was around “orange zones” identified by staff, like lounges, where clinicians in direct contact with patients may risk infecting unprotected staff. Such areas were made safer with behavioral protocols as well as architectural workarounds.
The hospital was able to convert 260 medical-surgical rooms in the Guggenheim Pavilion (1992, by Pei Cobb Freed & Partners) to infection-isolating rooms by installing fans that push room air outside through HEPA filters and exhaust vents that replace window panes. Equipment, pumps, and IV drips were moved into corridors, where they could be monitored by staff without exposure to contagion. And clear plastic film was stretched across metal studs in opened walls, allowing views into the rooms from the nursing stations.
Everyone involved recognized that such on-the-fly adaptation, while heroic, is far from ideal. With such shared guidance, MASS and other architects are beginning to assemble a roadmap to the future as health care runs as fast as it can into uncharted territory.
Looking for quick answers on architecture and design topics?
Try Ask RECORD, our new smart AI search tool.
Ask RECORD →
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!

