Pandemic Shifts Profession’s Focus to Health Care

Over the last several months, the COVID-19 pandemic has upended almost every aspect of day-to-day life, infecting millions of people across the globe, hundreds of thousands of whom have died. Many in the architecture, engineering, and construction industry have turned their focus to the rapid delivery of health-care facilities, to treat the ill and attempt to stave off the pandemic’s spread, and much of that work has been concentrated in coronavirus hot spots like New York.
Initial projections indicated that the largest city in the U.S. would need tens of thousands of additional hospital beds for the infected. Hospital systems married their in-house facilities staffs with architects and engineers to quickly assess how they might accommodate the expected influx. New York–based medical center NYU Langone Health, for example, retrofitted some older buildings to serve both contagious and noncontagious patients. A decommissioned structure was built out for large-scale coronavirus testing; a conference room became a staff testing center.

For many hospitals, an early goal was to fit out as many rooms as possible to Airborne Infection Isolation (AII) standards, a time-consuming and involved process. Using negative-pressure ventilation, and exhaust that is not recirculated, AII rooms prevent people nearby from being exposed to the airborne virus. But as updated guidance emerged from the U.S. Centers for Disease Control that the virus generally does not hang in air (rather, it clings to larger droplets that quickly precipitate), centers shifted to reserve AII rooms for only the most serious COVID-19 patients, whose treatment produces high quantities of virus-carrying vapor.
In adapting existing spaces to handle the coronavirus, “what you need is distancing,” says Chris Scovel, a director at Boston-based nonprofit MASS Design Group. “You try to isolate beds and provide quite generous corridors.” In addition, says MASS founding principal Michael Murphy, facilities need to have “protocols on surface infection and staff and patient separation,” such as infectious-disease areas sealed off and entered through vestibules.
Strategies derived from treatment centers built in places pummeled by the most serious contagious outbreaks in the world, such as tuberculosis, are embodied in guidance for architects that MASS is developing, with input from medical and public-health experts. The firm’s first publication outlines a tent-clinic prototype, with features that can also be applied to existing buildings. The design emulates AII best practices for ventilation by mounting a simple, screened exhaust vent at bed height. With supply air-fed from above, the vent removes contaminants before they can contact the health-care worker.

Other lessons come from hospitals in the U.S., like Rush University Medical Center. Recognizing the possibility of a pandemic or other mass casualty event, the Chicago institution opened the Robert R. McCormick Foundation Center for Advanced Emergency Response in 2012. The Perkins and Will–designed building includes an expansive covered sally port, within which ambulances deliver patients, that can be sealed off by overhead doors. In the current COVID-19 crisis, tents have been erected within the sally port to assess incoming patients. (Hospitals are increasingly using such tents to separate the possibly infected from staff and non-infected patients.) The emergency department can be divided into three pods, each of which can be deployed to isolate the contagious. Two of the pods are now being used for coronavirus intake. The hospital has also set up beds in its expansive lobby for less-acute patients—a contingency that the architects anticipated by installing access to power and utilities in the columns.

Several cities have addressed the surge in demand with rapidly assembled “field hospitals.” The U.S. Army Corps of Engineers installed beds in New York’s Jacob K. Javits Convention Center (more than 2000 were planned), and other temporary facilities have gone up in Los Angeles, Chicago, and Detroit.
Looking for quick answers on architecture and design topics?
Try Ask RECORD, our new smart AI search tool.
Ask RECORD →
The Boldt Company, a contractor in Appleton, Wisconsin, is prefabricating modular structures, designed by the firm HGA, that meet the need for speed without the sanitation and ventilation problems of tents. STAAT Mod, as the units are called, can be delivered on a standard truck trailer. They contain two finished patient rooms and a bathroom, along with medical and HVAC infrastructure that meet the negative-pressure standards for AII rooms.
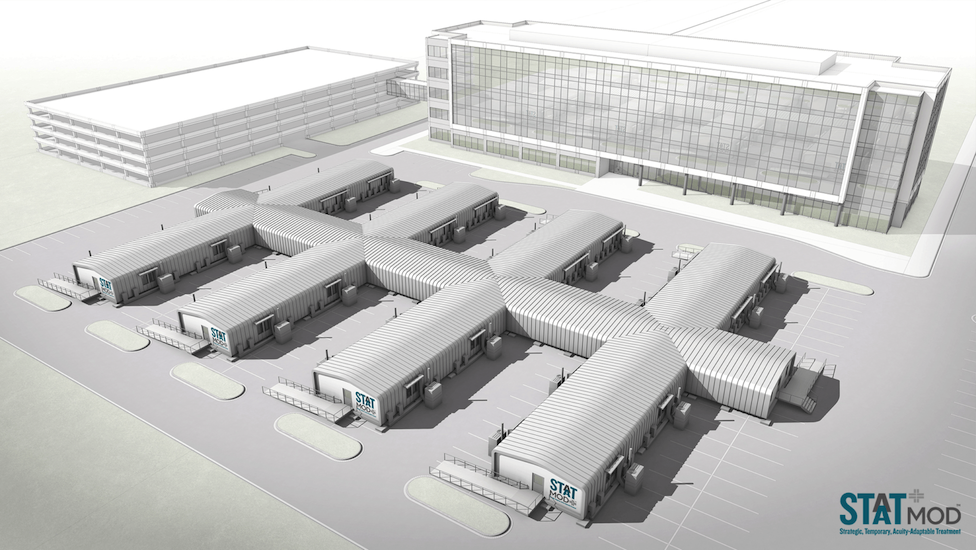
Virtual reality simulations allowed health-care professionals and HGA process engineers to weigh in on the validity of the designs, even as social-distancing orders precluded in-person meetings and the construction of physical prototypes. Projects are currently under way at four sites, with the first 16-bed configuration planned to be operational the first week of May.
Even as some cities are “flattening the curve” of rising cases, there seems little reason to slacken efforts to adapt hospitals to better manage such an unpredictable contagion. The next pandemic—or a rebound of the current one—could be just around the corner.
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!