From the RECORD Archives: ‘The Goldberg Effect’
In 2013, a vociferous preservation campaign tried to rescue Chicago’s Prentice Women’s Hospital from the wrecking ball. Petitions, signed by starchitects including Frank Gehry and Jeanne Gang, were circulated; landmark designations were sought; and last-ditch transformation schemes were proposed. But none of it was enough—and demolition completed in early 2015. Bertrand Goldberg’s clover-shaped tower was deemed too fragile to accommodate the state-of-the-art biomedical research center Northwestern University envisioned in its place. Admittedly, the building’s structural capacity was sacrificed, but for good reason, according to its designer: by assigning all lab and administrative equipment to the hospital’s rectilinear podium, Goldberg brought patients closer to nurses than ever before in the column-free quadrants above it. But this once headily futuristic and humanized vision for health care became an era-defining quirk that was not sustainable in the long term. (Indeed, the Perkins+Will–designed replacement reverted to linear layouts.) Readers who miss the old Prentice can rest assured that some of its siblings are still in use, including St. Joseph Hospital in Tacoma and St. Mary’s Hospital in Milwaukee. Together, the trio made an appearance in “the Goldberg Effect,” an article in the July 1976 edition of RECORD, which traced how the architect leveraged innovative engineering to rethink what a hospital should be.
Editor’s note: This article has been condensed for ease of online reading but reflects the original text.

© Architectural Record, July 1976. Click to enlarge
“The Goldberg Effect”
[No Author Attributed]
Architectural Record, July 1976
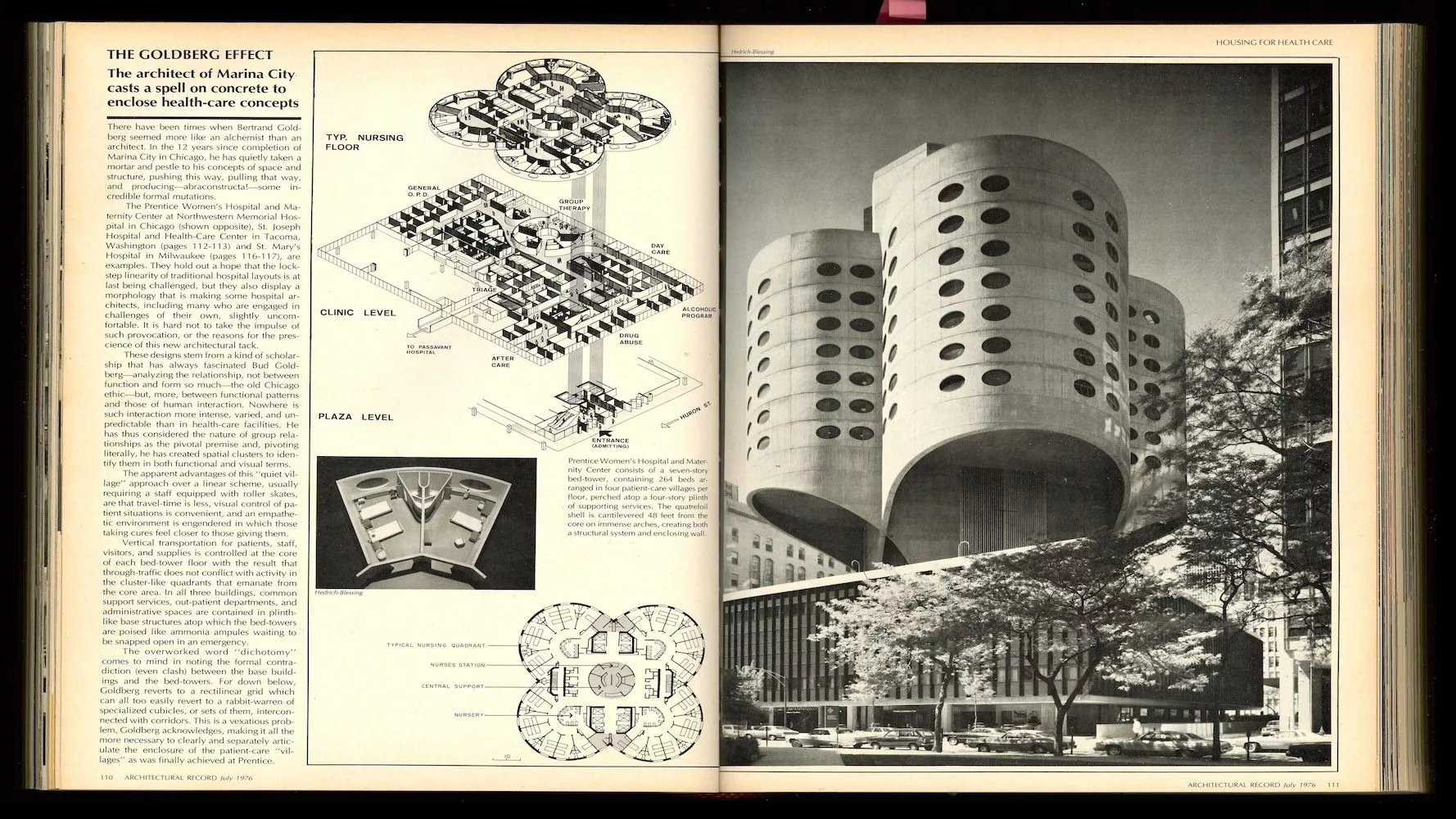
The architect of Marina City casts a spell on concrete to enclose health-care concepts.
There have been times when Bertrand Goldberg seemed more like an alchemist than an architect. In the 12 years since completion of Marina City in Chicago, he has quietly taken a mortar and pestle to his concepts of space and structure, pushing this way, pulling that way, and producing—abraconstructa!—some incredible formal mutations.
The Prentice Women’s Hospital and Maternity Center at Northwestern Memorial Hospital in Chicago, St. Joseph Hospital and Health-Care Center in Tacoma, Washington, and St. Mary’s Hospital in Milwaukee, are examples. They hold out a hope that the lockstep linearity of traditional hospital layouts is at last being challenged, but they also display a morphology that is making some hospital architects, including many who are engaged in challenges of their own, slightly uncomfortable. It is hard not to take the impulse of such provocation, or the reasons for the prescience of this new architectural tack.
These designs stem from a kind of scholarship that has always fascinated Bud Goldberg—analyzing the relationship, not between function and form so much—the old Chicago ethic—but more, between functional patterns and those of human interaction. Nowhere is such interaction more intense, varied, and unpredictable than in health-care facilities. He has thus considered the nature of group relationships as the pivotal premise and, pivoting literally, he has created spatial clusters to identify them in both functional and visual terms.

© Architectural Record, July 1976. Photos by Hedrich-Blessing
The apparent advantages of this “quiet village” approach over a linear scheme, usually requiring a staff equipped with roller skates, are that travel-time is less, visual control of patient situations is convenient, and an empathetic environment is engendered in which those taking cures feel closer to those giving them.
Vertical transportation for patients, staff, visitors and supplies is controlled at the core of each bed-tower floor with the result that through-traffic does not conflict with activity in cluster-like quadrants that emanate from the core area. In all three buildings, common support devices, out-patient departments, and administrative spaces are contained in plinth-like base structures atop which the bed-towers are poised like ammonia ampules waiting to be snapped open in an emergency.
The overworked word “dichotomy” comes to mind in noting the formal contradiction (even clash) between the base buildings and the bed-towers. For down below, Goldberg reverts to a rectilinear grid which can all too easily revert to a rabbit-warren of specialized cubicles, or sets of them, interconnected with corridors. This is a vexatious problem, Goldberg acknowledges, making it all the more necessary to clearly and separately articulate the enclosure of the patient-care “villages” as was finally achieved at Prentice.
Here an ingenious computer-calculated cantilever of monolithic lightweight concrete shells billows outward for 48 feet beyond the shear walls of the bed-tower cores containing stairs and elevators. The patient rooms in the tower’s seven stories, their plan formed by four intersecting circles like a four-leaf clover, are not only insulated from traffic noise but aloof from the frenzied variety of the goings-on in the four-story base. These house administrative and physicians’ offices, files, a psychiatric outpatient department, therapy, surgery, labor, delivery, and intensive care units for infants.
In a number of important respects, Goldberg hit the nail on the head with this shell configuration for the tower. For one thing, in the context of his “village” concept, the shell allows much more flexibility than would the typical post-and-beam structure. Another clincher is the economy of the system. For $13.50 per square foot, Goldberg gets structure, walls, and his unusual elliptical windows called “visional panels” all at once—a lot cheaper than a good glass curtainwall, which would normally come in at around $15 per square foot without the cost of the columns and beams backing it up. This alternative reduced Prentice’s over-all cost to about $57 per square foot, which is a bargain compared to the $75 per square foot (and up) normally associated with this building type. Front-end savings come by re-using a minimal number of forms; long-term savings are projected because the close-packed character of the structure and space cuts down on fuel consumption and mechanical runs while the thickness of the shell/wall—15 inches for the first three stories, 10 inches for the upper four—reduces thermal load.

© Architectural Record, July 1976. Photos by Tom Upper (left), Richards Studios (right)
Goldberg is enthusiastic about the construction method he has developed in these buildings. “The cost of form erection is approximately the same with flat forms in conventional building as our curved forms,” he points out. “The curved ones have an inevitable way of being put together, whereas the straight ones frequently require some amount of layout. But if you have enough re-use of the forms, then the costs drop down very low. In Marina City, for example, we had as many as 80 re-uses of the same form. Form cost is the one-time cost of the material plus the cost of your original layout.”
Looking for quick answers on architecture and design topics?
Try Ask RECORD, our new smart AI search tool.
Ask RECORD →
At St. Joseph, which preceded Prentice and is unlike it mainly because the shell/wall is supported on columns rather than being cantilevered from the core, the cost of the curvilinear shell was so minor a portion of the total that it came in well below the cost of conventional hospital design—about $47 per square foot.
The difference in shape between Prentice and St. Joseph lies in the fact that at St. Joseph the walls are “corrugated” as opposed to the radial shape of the Prentice quatrefoil. The columns supporting the corrugation, which is slightly cantilevered from them, coincide with the exterior plumbing runs of the inpatient rooms of the bed-tower, and they are designed to take lateral vibration—rather like shock absorbers in this earthquake-prone region. Loads are transferred to the foundation from the corrugated shell by way of conical column caps. This continuity and plasticity of material and force reads out dramatically in the over-all configuration of the building as the columns gently taper earthward.
In contrast, the curved quadrants at Prentice are completely core-supported, thus abridging the functional and formal contradiction, mentioned earlier, between the bed-tower and base structure. At St. Joseph, for example, it was discovered that where the tower columns entered the base there was chaos because the column structure of the base itself interfered and the columns of the two different systems often came very close together. Naturally, as far as activities in the base structure were concerned, layouts and spatial clarity tended to become confused. This is why Prentice called for a core-supported cantilevered shell. “We found that we were able to spring these shells from the core by paying a price only for the temporary support required to construct the two lower floors which, when completed, were self-supporting and enabled us to proceed quickly with pouring the shell above,” says Goldberg.
He had tried before to find such a cantilevered solution, realizing the complications brought on by the conflicting column systems of the tower and plinth at St. Joseph and St. Mary’s. The engineering proof was highly intricate, however, and it took many months of coddling his in-house computer bank—“very anthropomorphic machine,” he says—before an adequately strong shell could be worked out.
Here is how the solution came about. The first floor of the bed-tower, which is 55 feet from the roof of the plinth, gives way to the shell walls, rising 92 feet. The four cantilevered sections, emanating from the core area, intersect in a system of cylindrical arches that carry the forces into the walls of the core shaftways, which were engineered to receive loads and to act as wind bracing, this latter function needing no supplementary reinforcement. Because of the superior stress characteristics of the shell, the cantilever was accomplished from core walls of typical 12-inch thickness.

© Architectural Record, July 1976. Photos by Russ Camack (left), Hedrich-Blessing (right)
At St. Mary’s Hospital in Milwaukee, the design of which was concluded slightly before the engineering breakthrough making possible the Prentice parti, there is a somewhat different modification in that, unlike either St. Joseph or Prentice, such large floor areas which were specified by the client that the column- or core-supported technique of the other two jobs was not economically feasible. Yet St. Mary’s was taken with and wanted a simulation of Goldberg’s village-y clustering of bed space around the nursing stations. What they have as a result is, again, a plinth of support services, this one 150- by 300-feet and three-stories -high, atop which is a five-story bed-tower. Here the floor loads are supported by a system of columns radially arrayed around a central column located smack-dab in the middle of each nursing substation.
The elliptical windows that appear in the other two buildings were dispensed with in this one because of the inherent disparity between the structural system and the non-structural enfolding walls—walls which, in the other two, remember, were simultaneously structural. At St. Mary’s, the walls are simply undulating curtains, reflecting the internal disposition of bed space. Hence the windows are square, as if to underscore the conventional structural system of columns. Why? Because there are not the stresses involved here that apply in the shells of St. Joseph and Prentice, and their elliptical windows were used to underscore that flow of stress. These “vision panels,” which give a certain porthole and stateroom quality to the patient-care units, lessen the possibility of cracking, which often occurs at the corners of square windows in a structural concrete wall. Also, less reinforcing was required around the openings, thus incurring some savings. But at St. Mary’s, “where a new shape is using an old structural form,” as Goldberg puts it, the square window was a way of telling the truth about the compromise he had to make.
“My approach in this work goes back to an absolutely ancient relationship, such as existed in the open wards of past centuries. What we are trying to restore is the give-and-take, the come-and-go, between the very ill person and the very concerned care group, and we do this on the premise that people, who cannot afford to be casually ill, have a right to a mode and a mood of treatment that goes beyond the old story, routine in the familiar linear layout, of people running long distances to deliver a glass of water or making the pill run,” says Bertrand Goldberg sardonically. “Cutting hospitals out of linear yard goods may be acceptable when you are interested in structural relativity for functions not directly related to patients but, for them, human relativity is a prod to recovery and, from it, we derive not only a new pattern of care and concern but a more telling pattern of space.”
As controversial as these designs are among those still preoccupied with cutting out “linear yard goods,” they at least bring architecture closer to medicine’s focal contribution to society. As Dr. Edmund Pellegrino, chairman of Yale/New Haven Medical Center, puts it, “The sick person wants to know what is wrong, how he got that way, what will happen to him, whether he can be helped and how, and what it will cost in discomfort, money, and personal dignity.” It is a blend of competence and compassion, answering such questions. If the Goldberg Effect is only to dramatize the need for these qualities, he will have ventured an answer to be dealt with.
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!



